A simple HIV prevention cascade could be a powerful tool for advocates, policy makers and funders, researchers argue in The Lancet HIV. It could help us understand where the gaps in prevention are, to monitor implementation and to set meaningful targets.
Robin Schaefer of Imperial College London, Professor James Hargreaves of the London School of Hygiene and Tropical Medicine and colleagues aim to replicate the success of the HIV treatment cascade and UNAIDS’ 90-90-90 targets as advocacy and policy tools. “The HIV treatment cascade has shown how a unifying framework can become a driving force for programmes and policy nationally and internationally,” they say.
Other models of prevention cascades have been proposed before, sometimes specific to a particular prevention method (e.g. male circumcision or pre-exposure prophylaxis (PrEP)). But the authors believe that we need a framework that can be used across prevention methods, populations and programmes. To be widely used, it should be simple (only including the core steps and essential determinants) and measure those core steps in a standardised way.
They propose a generic HIV prevention cascade which recognises that the use of prevention methods is behavioural, affected by social and structural forces.
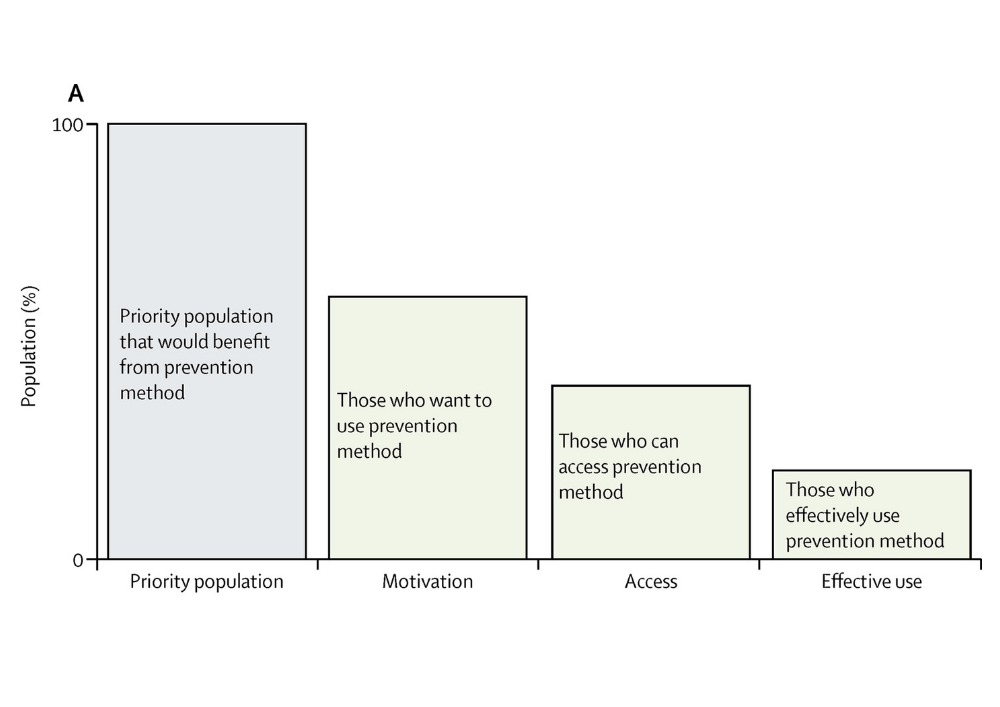
- The first block represents the population that would benefit from the prevention method (for example, men who have sex with men, or women aged 15-30 years).
- The second block represents those who are motivated to use the prevention method (for example, wanting to take PrEP). Motivation is likely to be influenced by knowledge, social norms and perception of being at risk of HIV infection.
- The third block represents the proportion of the population who can access the prevention method. High costs, or inappropriate or inaccessible services could result in a lack of access.
- The last block represents those who are effectively using the prevention method. Gaps here could reflect inconsistent use or a sexual partner’s refusal to allow the prevention method to be used.
The authors give a practical example of how this cascade can be used for a specific method in a specific population – condom use among adult men in a province of eastern Zimbabwe.
- Population: 100%. The denominator is HIV-negative men who report multiple, casual or concurrent sexual partners.
- Motivation: 33%. A survey showed that the principle gaps in motivation related to perceiving condoms to be socially unacceptable or reducing sexual pleasure.
- Access: 33%. In the survey, all men who had motivation to use condoms knew how to obtain them.
- Effective use: 17%. Only half of those who had motivation and access reported consistent condom use over the last two weeks. The main explanation of inconsistent use was a lack of partner support. In contrast, very few men reported problems with self-efficacy to use condoms.
A similar cascade for women in the same area highlighted different gaps. Far more women than men were motivated to use condoms, but a lack of partner support was even more important a factor preventing effective use. While most women could access condoms, a few could not.
Identifying the reasons for gaps in the cascade could help in the development of interventions. In this example, community-based interventions to make condoms more socially acceptable would appear to be a priority. Couples counselling and strengthening women’s rights might have an impact on effective use.
Schaefer and colleagues say that whereas this cascade covered a single prevention method, data could be combined in a combination prevention cascade. For example, this would show the proportion of people motivated to use any one of a number of prevention methods.
One of the challenges with the cascade is of having appropriate and accurate data to measure motivation, access and effective use. Relevant indicators are not routinely collected and may not even be available from research studies. To take the condom cascade in Zimbabwe as an example, the authors could not find data on motivation to use condoms specifically. Instead, individuals were classified as motivated if they perceived themselves to be at risk of HIV.
The authors have excluded additional steps for which it would be even harder to collect or calculate data – such as the number of HIV infections averted.
They believe that its simple three-step structure means that it can be widely used, in different settings and for different prevention methods. “The cascade can be used for advocacy, routine monitoring, and strategic planning,” they say.
Schaefer R et al. HIV prevention cascades: a unifying framework to replicate the successes of treatment cascades. Lancet HIV 6: 60-66, 2019. (Article).
Image credit: The core steps of the prevention method cascade graph, from the paper in The Lancet HIV.