Most health problems in people living with HIV in two large cohorts can be classified in six clusters, with cardiovascular disease, metabolic problems, sexually transmitted infections and mental health conditions being the most common in Britain, Ireland and the Netherlands, according to research published in the journal Open Forum Infectious Diseases last month.
The clusters identified in the study reveal the major non-HIV medical needs of people living with HIV, especially older adults, and the needs for prevention of ill health.
Findings from the study were also presented at the Conference on Retroviruses and Opportunistic Infections (CROI) in Seattle earlier this month.
Two cohorts were analysed in the study, which was designed to detect patterns in potentially preventable co-morbidities in people living with HIV and to provide information to help better targeting of interventions and a better understanding of shared pathophysiology of co-morbidities.
The POPPY cohort consisted of 699 people with HIV aged 50 or over and 374 younger people with HIV, receiving care in the United Kingdom and Ireland. Eighty-five per cent of the cohort was male, the median age was 52, 15.9% were black African, and 76% were men who have sex with men. Participants had been living with HIV for a median of 13.2 years, 97.5% were on antiretroviral treatment and 89.9% had a viral load below 50 copies/ml. The median age in the over-50 segment of the cohort was 57 years and duration of HIV infection was slightly longer (15.8 years) but in other respects the older segment was demographically similar to the overall cohort.
The AGEhIV cohort consisted of 598 people living with HIV aged 45 and over receiving care in the Netherlands. Demographic characteristics and HIV history were very similar to the overall POPPY cohort.
Co-morbidities were captured through a structured interview cross-checked against medical records. There were a few differences in the list of co-morbidities asked about in the two cohorts.
The most common single co-morbidities in POPPY were gonorrhoea (42.6%), syphilis (30.4%), depression (32.4%) and dyslipidaemia (27.3%). In AGEhIV the most common co-morbidities were hypertension (43.1%), osteopenia/osteoporosis (42.6%), lipodystrophy/lipoatrophy (32.1%) and candidiasis (31.9%). In both cohorts, people reported a median of five co-morbidities.
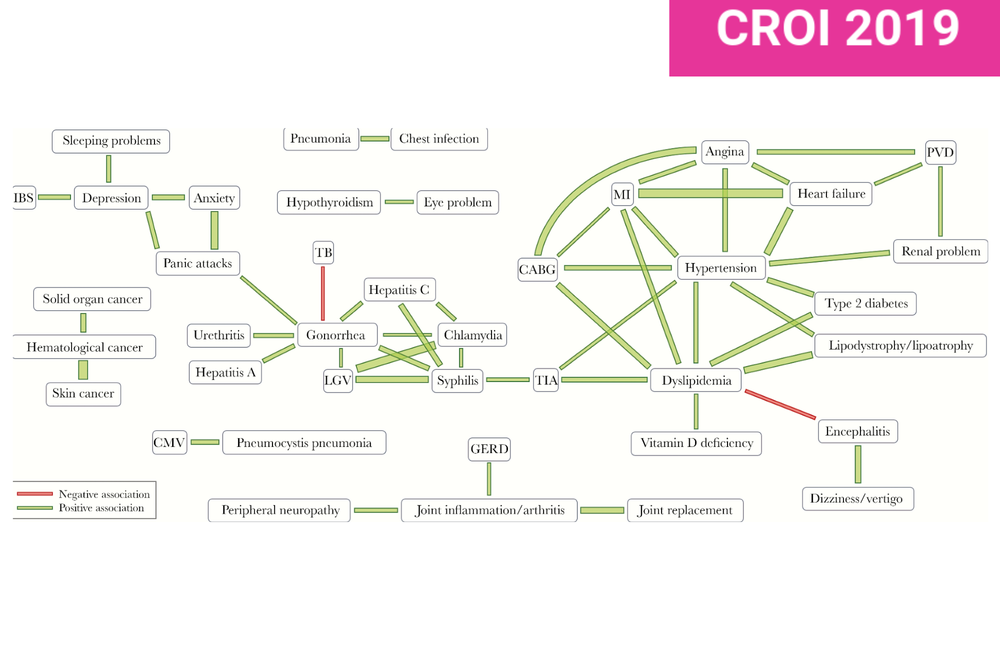
The researchers analysed the relationship between co-morbidities to identify conditions that are more likely to occur together in the same person than would be expected by chance alone. In the POPPY cohort, they identified six clusters:
- cardiovascular (angina, coronary bypass surgery, heart attack, heart failure, high blood pressure, peripheral vascular disease, end stage kidney disease)
- sexually transmitted diseases (gonorrhoea, lymphogranuloma venereum [LGV], chlamydia, hepatitis C)
- mental health (depression, anxiety, panic attacks)
- cancers (blood cancers, skin cancer, solid organ cancer)
- metabolic (abnormal lipids, lipodystrophy, high blood pressure)
- chest and other infections (cytomegalovirus [CMV], pneumonia, dizziness/vertigo, asthma/bronchitis/chronic obstructive pulmonary disease [COPD], chest infection).
Similar clusters were seen in AGEhIV.
Moreover, in the POPPY study:
- People with a higher burden of cardiovascular disease tended to have a lower burden of sexually transmitted infections, and vice versa.
- Depression was associated with sleeping problems and irritable bowel syndrome.
- Greater severity of mental health problems was strongly associated with severity of all other health patterns, but especially cancers and chest and other infections.
- In the older people in the POPPY cohort, greater cardiovascular disease severity was associated with greater severity of mental health, metabolic and asthma scores.
- In older individuals, panic attacks were associated with asthma/bronchitis/COPD.
In the AGEhIV study:
- Cardiovascular disease was most strongly associated with a past history of AIDS-defining conditions.
- Depression was associated with neurological problems such as dizziness/vertigo.
- More severe general health problems were strongly associated with greater severity of cardiovascular disease, chest or liver disorders, and mental health or neurological problems.
The investigators say that their findings demonstrate that “comorbidities do not co-occur at random, and in general, are likely to cluster in specific patterns, some which are consistent across different cohorts.”
Although some of the clusters – such as cardiovascular disease and metabolic problems – are well recognised and have common pathologies, other patterns are less well established, they say. The strong association between mental health and neurological problems deserves more investigation, as do the associations between mental health disorders and cardiovascular disease, metabolic problems and sexually transmitted infections.
Looking at the POPPY cohort alone, the researchers also found that different co-morbidity clusters were associated with different risk factors. For example, prior AIDS was associated with cardiovascular disease, mental health problems, cancers and chest or other infections, but not with metabolic problems. People with a history of injecting drug use, who formed about 10% of the cohort, were less likely to have co-morbidities except for mental health problems or sexually transmitted infections.
Surprisingly, current or former smoking was not associated with any co-morbidity cluster, and nor was nadir CD4 cell count.
Image: Graphic from the study showing significant nonrandom associations between co-morbidities in the POPPY cohort.
De Francesco D et al. Patterns of co-occurring comorbidities in people living with HIV. Open Forum Infectious Disease, 2019, DOI: 10.1093/ofid/ofy272.
De Francesco D et al. Impact and determinants of comorbidity clusters in people living with HIV. Conference on Retroviruses and Opportunistic Infections, Seattle, abstract 697, 2019.